What Are The Main Causes Of Posterior Calcaneal Spur
:origin()/pre14/f8b9/th/pre/f/2012/020/e/8/skadi_fairy_queen_fanart_by_calcaneus-d4n0dmb.jpg)
Overview
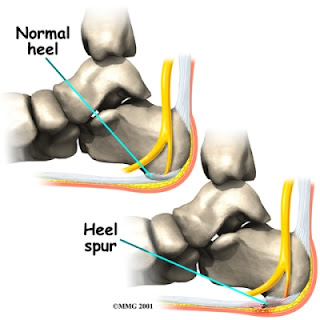
Heel spurs refer to the abnormal accumulation of calcium deposits on the heel of the foot. Vigorous, repetitive movements often result in the formation of heel spurs, but inflammatory diseases (e.g., arthritis) may also increase the occurrence of painful heel spurs. Treatments that have proven to be effective for heel spurs include injections that contain a combination of steroids and anesthesia as well as radiofrequency ablation. However, a bone spur that begins to protrude excessively may need to be removed through surgery.
Causes
There exists a membrane that covers most of the bone along the heel. When this membrane gets torn repeatedly due to straining of the muscles in the foot, the calcium deposits that lead to heel spurs are more likely to occur.
Symptoms
More often than not, heel spurs have no signs or symptoms, and you don?t feel any pain. This is because heel spurs aren?t pointy or sharp pieces of bone, contrary to common belief. Heel spurs don?t cut tissue every time movement occurs; they?re actually deposits of calcium on bone set in place by the body?s normal bone-forming mechanisms. This means they?re smooth and flat, just like all other bones. Because there?s already tissue present at the site of a heel spur, sometimes that area and the surrounding tissue get inflamed, leading to a number of symptoms, such as chronic heel pain that occurs when jogging or walking.
Diagnosis
A Heel Spur diagnosis is made when an X-ray shows a hook of bone protruding from the bottom of the foot at the point where the plantar fascia is attached to the heel bone. The plantar fascia is the thick, connective tissue that runs from the calcaneus (heel bone) to the ball of the foot. This strong and tight tissue helps maintain the arch of the foot. It is also one of the major transmitters of weight across the foot as you walk or run. In other words, tremendous stress is placed on the plantar fascia.
Non Surgical Treatment
Diathermy treatment uses an electrical current to produce heat that sedates the inflamed tissues. The ultrasound device sends sound waves into the heel and sets up a massaging action that stimulates blood circulation. Treatment with a whirlpool bath involves placing the foot directly into the jetting stream. Orthopedic molds and appliances, such as orthotics, are designed by foot specialists for use inside the shoe to eliminate irritation to the heel when the patient stands or walks. When those appliances are used, the spur (in effect) floats on air. At the same time, the body's weight is transferred forward from the tender spot.
Surgical Treatment
In some cases, heel spurs are removed by surgery after an X-ray. While the surgery is typically effective, it?s a timely and expensive procedure. Even after surgery, heel spurs can re-form if the patient continues the lifestyle that led to the problem. These reasons are why most people who develop painful heel spurs begin looking for natural remedies for joint and bone pain. Surgery isn?t required to cure a heel spur. In fact, more than 90 percent of people get better with nonsurgical treatments. If nonsurgical methods fail to treat symptoms of heel spurs after 12 months, surgery may be necessary to alleviate pain and restore mobility.
Find Out How To Treat Bursitis In Ball Of Foot
Overview
There are about 160 bursae in the human body. These little, fluid-filled sacs cushion pressure and lubricate points between our bones, tendons, and muscles near our joints. The bursae are lined with synovial cells. Synovial cells produce a lubricant that reduces friction. This cushioning and lubrication allows our joints to move easily. When a person has bursitis, inflammation of the bursa, movement or pressure is painful. Overuse, injury and sometimes an infection from gout or rheumatoid arthritis may cause bursitis.
Causes
Bursitis, tendinitis, and other soft tissue rheumatic syndromes typically result from one or more factors. These include: Play or work activities that cause overuse or injury to the joint areas Incorrect posture Stress on the soft tissues from an abnormal or poorly positioned joint or bone (such as leg length differences or arthritis in a joint) Other diseases or conditions (rheumatoid arthritis, gout, psoriasis, thyroid disease, or an unusual drug reaction) Infection.
Symptoms
Symptoms include pain at the back of the heel, especially when running uphill or on soft surfaces. There will be tenderness and swelling at the back of the heel which may make it difficult to wear certain shoes. When pressing in with the fingers both sides are the back of the heel a spongy resistance may be felt.
Diagnosis
When a patient has pain in a joint, a careful physical examination is needed to determine what type of movement is affected and if there is any swelling present. Bursitis will not show up on x-rays, although sometimes there are also calcium deposits in the joint that can be seen. Inserting a thin needle into the affected bursa and removing (aspirating) some of the synovial fluid for examination can confirm the diagnosis. In most cases, the fluid will not be clear. It can be tested for the presence of microorganisms, which would indicate an infection, and crystals, which could indicate gout. In instances where the diagnosis is difficult, a local anesthetic (a drug that numbs the area) is injected into the painful spot. If the discomfort stops temporarily, then bursitis is probably the correct diagnosis.
Non Surgical Treatment
The patient with retrocalcaneal bursitis should be instructed to apply ice to the posterior heel and ankle in the acute period of the bursitis. Icing can be performed several times a day, for 15-20 minutes each. Some clinicians also advocate the use of contrast baths. Gradual progressive stretching of the Achilles tendon may help relieve impingement on the subtendinous bursa and can be performed in the following manner. Stand in front of a wall, with the affected foot flat on the floor. Lean forward toward the wall until a gentle stretching is felt within the ipsilateral Achilles tendon. Maintain the stretch for 20-60 seconds and then relax. Perform the stretches with the knee extended and then again with the knee flexed. To maximize the benefit of the stretching program, repeat the above steps for several stretches per set, several times daily. Avoid ballistic (ie, abrupt, jerking) stretches. Other treatment options are microcurrent therapy and corticosteriod injection into the retrocalcaneal bursa. If conservation treatment fails then surgery is indicated.
Surgical Treatment
Surgery. Though rare, particularly challenging cases of retrocalcaneal bursitis might warrant a bursectomy, in which the troublesome bursa is removed from the back of the ankle. Surgery can be effective, but operating on this boney area can cause complications, such as trouble with skin healing at the incision site. In addition to removing the bursa, a doctor may use the surgery to treat another condition associated with the retrocalcaneal bursitis. For example, a surgeon may remove a sliver of bone from the back of the heel to alter foot mechanics and reduce future friction. Any bone spurs located where the Achilles attaches to the heel may also be removed. Regardless of the conservative treatment that is provided, it is important to wait until all pain and swelling around the back of the heel is gone before resuming activities. This may take several weeks. Once symptoms are gone, a patient may make a gradual return to his or her activity level before their bursitis symptoms began. Returning to activities that cause friction or stress on the bursa before it is healed will likely cause bursitis symptoms to flare up again.
There are about 160 bursae in the human body. These little, fluid-filled sacs cushion pressure and lubricate points between our bones, tendons, and muscles near our joints. The bursae are lined with synovial cells. Synovial cells produce a lubricant that reduces friction. This cushioning and lubrication allows our joints to move easily. When a person has bursitis, inflammation of the bursa, movement or pressure is painful. Overuse, injury and sometimes an infection from gout or rheumatoid arthritis may cause bursitis.
Causes
Bursitis, tendinitis, and other soft tissue rheumatic syndromes typically result from one or more factors. These include: Play or work activities that cause overuse or injury to the joint areas Incorrect posture Stress on the soft tissues from an abnormal or poorly positioned joint or bone (such as leg length differences or arthritis in a joint) Other diseases or conditions (rheumatoid arthritis, gout, psoriasis, thyroid disease, or an unusual drug reaction) Infection.
Symptoms
Symptoms include pain at the back of the heel, especially when running uphill or on soft surfaces. There will be tenderness and swelling at the back of the heel which may make it difficult to wear certain shoes. When pressing in with the fingers both sides are the back of the heel a spongy resistance may be felt.
Diagnosis
When a patient has pain in a joint, a careful physical examination is needed to determine what type of movement is affected and if there is any swelling present. Bursitis will not show up on x-rays, although sometimes there are also calcium deposits in the joint that can be seen. Inserting a thin needle into the affected bursa and removing (aspirating) some of the synovial fluid for examination can confirm the diagnosis. In most cases, the fluid will not be clear. It can be tested for the presence of microorganisms, which would indicate an infection, and crystals, which could indicate gout. In instances where the diagnosis is difficult, a local anesthetic (a drug that numbs the area) is injected into the painful spot. If the discomfort stops temporarily, then bursitis is probably the correct diagnosis.
Non Surgical Treatment
The patient with retrocalcaneal bursitis should be instructed to apply ice to the posterior heel and ankle in the acute period of the bursitis. Icing can be performed several times a day, for 15-20 minutes each. Some clinicians also advocate the use of contrast baths. Gradual progressive stretching of the Achilles tendon may help relieve impingement on the subtendinous bursa and can be performed in the following manner. Stand in front of a wall, with the affected foot flat on the floor. Lean forward toward the wall until a gentle stretching is felt within the ipsilateral Achilles tendon. Maintain the stretch for 20-60 seconds and then relax. Perform the stretches with the knee extended and then again with the knee flexed. To maximize the benefit of the stretching program, repeat the above steps for several stretches per set, several times daily. Avoid ballistic (ie, abrupt, jerking) stretches. Other treatment options are microcurrent therapy and corticosteriod injection into the retrocalcaneal bursa. If conservation treatment fails then surgery is indicated.
Surgical Treatment
Surgery. Though rare, particularly challenging cases of retrocalcaneal bursitis might warrant a bursectomy, in which the troublesome bursa is removed from the back of the ankle. Surgery can be effective, but operating on this boney area can cause complications, such as trouble with skin healing at the incision site. In addition to removing the bursa, a doctor may use the surgery to treat another condition associated with the retrocalcaneal bursitis. For example, a surgeon may remove a sliver of bone from the back of the heel to alter foot mechanics and reduce future friction. Any bone spurs located where the Achilles attaches to the heel may also be removed. Regardless of the conservative treatment that is provided, it is important to wait until all pain and swelling around the back of the heel is gone before resuming activities. This may take several weeks. Once symptoms are gone, a patient may make a gradual return to his or her activity level before their bursitis symptoms began. Returning to activities that cause friction or stress on the bursa before it is healed will likely cause bursitis symptoms to flare up again.
Treatment For Hammer Toes Pain
 Overview
Overview
Hammer toes are classified based on the mobility of the toe joints. There are two types. Flexible and rigid. In a flexible Hammer toe, the joint has the ability to move. This type of hammer toe can be straightened manually. A rigid hammer toe does not have that same ability to move. Movement is very limited and can be extremely painful. This sometimes causes foot movement to become restricted leading to extra stress at the ball-of-the-foot, and possibly causing pain and the development of corns and calluses.
Causes
Hammertoes are most common in women, and a big part of this is poor shoe choices, which are a big factor in the development of many foot problems. Tight toe boxes and high heels are the biggest culprits. Genetics certainly plays a role in some cases of hammertoes, as does trauma, infection, arthritis, and certain neurological and muscle disorders. But most cases of contracted toes are associated with various biomechanical abnormalities in how a patient walks. This causes the muscles and tendons to be used excessively or improperly, which deforms the toes over time.
 Symptoms
Symptoms
Symptoms may include pain in the affected toe or toes when you wear shoes, making it hard or painful to walk. A corn or callus on the top of the joint caused by rubbing against the shoe. Swelling and redness of the skin over the joint. Trouble finding comfortable shoes.
Diagnosis
Hammertoes are progressive, they don?t go away by themselves and usually they will Hammer toes get worse over time. However, not all cases are alike, some hammertoes progress more rapidly than others. Once your foot and ankle surgeon has evaluated your hammertoes, a treatment plan can be developed that is suited to your needs.
Non Surgical Treatment
Orthotics are shoe inserts that can help correct mechanical foot-motion problems to correct pressure on your toe or toes and reduce pain. Changing shoes. You should seek out shoes that conform to the shape of your feet as much as possible and provide plenty of room in the toe box, ensuring that your toes are not pinched or squeezed. You should make sure that, while standing, there is a half inch of space for your longest toe at the end of each shoe. Make sure the ball of your foot fits comfortably in the widest part of the shoe. Feet normally swell during the course of the day, so shop for shoes at the end of the day, when your feet are at their largest. Don't be vain about your shoe size, sizes vary by brand, so concentrate on making certain your shoes are comfortable. Remember that your two feet are very likely to be different sizes and fit your shoe size to the larger foot. Low-heel shoes. High heels shift all your body weight onto your toes, tremendously increasing the pressure on them and the joints associated with them. Instead, wear shoes with low (less than two inches) or flat heels that fit your foot comfortably.
Surgical Treatment
Sometimes, if the deformity is severe enough or surgical modification is needed, the toe bones may be fused so that the toe does not bend. Buried wires are used to allow for the fusion to heal, and they remain in place after healing. Your skin is closed with fine sutures, which are typically removed seven to ten days after surgery. A dressing is used to help keep your toes in their new position. Dressings should not get wet or be removed. After surgery, your doctor may prescribe pain relievers, typically for the initial four to seven days. Most people heal completely within one month of surgery, with few complications, if any. Crutches or a cane may be needed to help you keep weight off your affected foot, depending on the procedure. Occasionally, patients receive a special post-op shoe or a walking boot that is to be worn during the healing process. Most people are able to shower normally after surgery, but must protect the dressing from getting wet. Many patients are allowed to resume driving within one week after the procedure, but care needs to be taken.
Bunions Causes Symptoms And Treatment Options
Overview
 Hallux Abducto Valgus, commonly called bunion, is a bony deformity affecting the angle of the joint at the base of the big toe. Some medical professionals believe that the condition is solely due to ill-fitting footwear, while others believe it is a genetic structural defect that can be exacerbated by shoes. Despite the varying opinions, the reality is that it is probably a combination of both factors. A bunion forms when pressure is applied to the side of the big toe, causing it to become inflamed and painful. The joint then protrudes, effectively making the foot wider. The second toe might then become displaced, which can cause a multitude of other issues like corn and callus development. The bunion joint will have a reduced range of motion and often ends up arthritic. The condition usually develops later in life.
Hallux Abducto Valgus, commonly called bunion, is a bony deformity affecting the angle of the joint at the base of the big toe. Some medical professionals believe that the condition is solely due to ill-fitting footwear, while others believe it is a genetic structural defect that can be exacerbated by shoes. Despite the varying opinions, the reality is that it is probably a combination of both factors. A bunion forms when pressure is applied to the side of the big toe, causing it to become inflamed and painful. The joint then protrudes, effectively making the foot wider. The second toe might then become displaced, which can cause a multitude of other issues like corn and callus development. The bunion joint will have a reduced range of motion and often ends up arthritic. The condition usually develops later in life.
Causes
Improper footwear. Podiatric physicians have long believed that narrow, poor-fitting shoes with a tight toe box tend to compress the end of the foot, leading to abnormal motion of the foot and pressure over the MTP joint. High-heeled shoes tend to add even more pressure to the toes, as the foot slides downward. Over time, continued pressure will squeeze the toes together, encouraging the deformity. Occupational hazards. Individuals whose jobs place undue stress on their feet are among those who complain of bunions. Ballet dancers, in particular, put great demands on their toes, and thus are often subject to bunions, however, they are not alone. Many professionals whose jobs require a great deal of standing or walking (teachers, police officers, doctors and nurses, etc.) and/or who are required to wear a particular type of shoe or boot as part of a uniform, also are at risk. Athletes such as runners or walkers, who utilize the wrong footwear, may also develop bunions.
Symptoms
If you have a bunion, you may have pain or stiffness of your big toe joint, swelling of your big toe joint, difficulty walking, difficulty finding shoes that fit. These symptoms may be caused by conditions other than bunions, but if you have any of these symptoms, see your doctor.
Diagnosis
When an x-ray of a bunion is taken, there is usually angulation between the first metatarsal bone and the bones of the big toe. There may also be angulation between the first and second metatarsal bones. These angular irregularities are the essence of most bunions. In general, surgery for bunions aims to correct such angular deformities.
Non Surgical Treatment
In the early stages of the formation of a bunion, soaking feet in warm water can provide temporary relief. The best way to alleviate the pain associated with bunions is to wear properly fitting shoes. Shoes designed with a high, wide toe box (toe area) are recommended for people suffering from forefoot disorders, such as bunions. Shoes with rocker soles will unload pressure to the bunion area. Orthotics are also recommended for this condition to provide extra comfort, support, and protection. Other conservative treatments include using forefoot products designed to accommodate and relieve bunions such as bunion shields, bunion night splints, and bunion bandages. These conservative treatments can limit the progression of the bunion formation, relieve pain and provide a healthy environment for the foot. 
Surgical Treatment
Research shows that 85% of people who have bunion corrections are satisfied with the results. However, a number of problems can arise. The big toe is usually stiffer than before. For most people this does not matter, but for athletes or dancers it is very important. As mentioned before, the big toe is slightly weaker with a bunion, and this transfers weight onto the ball of the foot. After bunion surgery, this transfer of weight can increase. Therefore, if you have pain under the ball of the foot ("metatarsalgia") it may be worse after bunion surgery, and it may also develop for the first time. Careful surgical technique can reduce this risk, but it cannot avoid it completely. Most people who develop metatarsalgia are comfortable with a simple insole in the shoe but occasionally surgery is required. In some people the big toe slowly tilts back toward the original position and occasionally this is bad enough to need to have the operation redone. On the other hand, the toe can tilt the other way, though much more rarely. Again, occasionally this is bad enough to need to have the operation redone. Infections in the wound, plaster problems and minor damage to the nerves of the toe can occur in any foot surgery. Usually these are minor problems that get better quickly. This may sound like a lot of possible problems, but in fact most people do not get them and are satisfied with their bunion surgery. However, this may help you to see how important it is to have any bunion surgery carried out by a properly trained and experienced foot and ankle surgeon.
Prevention
Wear insoles and well-fitting shoes to help slow down the progression of bunions and alleviate discomfort. Cushioning can also help alleviate discomfort. Consider wearing shoes with a wide toe box so they don't crowd your toes. Children can also develop bunions and should wear properly fitting shoes as their feet are still developing.
Overpronation Of The Foot
Overview
Over Pronation (Flat Feet) refers to the biomechanical shock-absorbing motion of the ankle, foot and lower leg. It is the natural inward flexing motion of the lower leg and ankle. Standing, walking, and running cause the ankle joint to pronate which in turn helps the body to absorb shock and allows it to control balance. An ankle joint that is too flexible causes more pronation than desired. This common condition is called Over- Pronation (sometimes referred to as "Flat Feet"). This foot condition places an extreme degree of strain on various connective tissues of the ankle, foot, and knee. If this condition is not addressed foot pain and toe deformities such as bunions and hammer toes (just to name a couple) may develop. Hip and lower back pain may also be residual results from this condition.
Causes
There are many possible causes for overpronation, but researchers have not yet determined one underlying cause. Hintermann states, Compensatory overpronation may occur for anatomical reasons, such as a tibia vara of 10 degrees or more, forefoot varus, leg length discrepancy, ligamentous laxity, or because of muscular weakness or tightness in the gastrocnemius and soleus muscles. Pronation can be influenced by sources outside of the body as well. Shoes have been shown to significantly influence pronation. Hintermann states that the same person can have different amounts of pronation just by using different running shoes. It is easily possible that the maximal ankle joint eversion movement is 31 degrees for one and 12 degrees for another running shoe.
Symptoms
With over pronation, sufferers are most likely to experience pain through the arch of the foot. A lack of stability is also a common complaint. Over pronation also causes the foot to turn outward during movement at the ankle, causing sufferers to walk along the inner portion of the foot. This not only can deliver serious pain through the heel and ankle, but it can also be the cause of pain in the knees or lower back as well. This condition also causes the arch to sink which places stress on the bones, ligaments, and tendons throughout the foot. This may yield other common conditions of foot pain such as plantar fasciitis and heel spurs.
Diagnosis
To easily get an idea of whether a person overpronates, look at the position and condition of certain structures in the feet and ankles when he/she stands still. When performing weight-bearing activities like walking or running, muscles and other soft tissue structures work to control gravity's effect and ground reaction forces to the joints. If the muscles of the leg, pelvis, and feet are working correctly, then the joints in these areas such as the knees, hips, and ankles will experience less stress. However, if the muscles and other soft tissues are not working efficiently, then structural changes and clues in the feet are visible and indicate habitual overpronation.
Non Surgical Treatment
Anti-Pronation Insoles provide a unique foot support system that aligns the lower body. The major cause of foot and leg pain is over pronation (rolling over of the feet) which causes excessive pressure on the muscles, ligaments and bones of the lower body. Running insoles treat the underlying cause of over pronation and prevent future occurrences of the associated foot or leg condition. A project conducted at the NIKE Sport Research Laboratory studied the effects of orthotics on rear foot movement in running. Nine well-trained runners who wore orthotics were chosen as subjects. The results of the study indicated that orthotics reduced rear foot movement by roughly one degree or approximately nine percent of the amount found in runners not using orthotics. The average reduction of the maximum velocity of pronation was fifteen percent. Thus this study indicates that orthotics and insoles control over pronation which will treat and prevent many sporting injuries.
Surgical Treatment
Depending on the severity of your condition, your surgeon may recommend one or more treatment options. Ultimately, however, it's YOUR decision as to which makes the most sense to you. There are many resources available online and elsewhere for you to research the various options and make an informed decision.
Over Pronation (Flat Feet) refers to the biomechanical shock-absorbing motion of the ankle, foot and lower leg. It is the natural inward flexing motion of the lower leg and ankle. Standing, walking, and running cause the ankle joint to pronate which in turn helps the body to absorb shock and allows it to control balance. An ankle joint that is too flexible causes more pronation than desired. This common condition is called Over- Pronation (sometimes referred to as "Flat Feet"). This foot condition places an extreme degree of strain on various connective tissues of the ankle, foot, and knee. If this condition is not addressed foot pain and toe deformities such as bunions and hammer toes (just to name a couple) may develop. Hip and lower back pain may also be residual results from this condition.
Causes
There are many possible causes for overpronation, but researchers have not yet determined one underlying cause. Hintermann states, Compensatory overpronation may occur for anatomical reasons, such as a tibia vara of 10 degrees or more, forefoot varus, leg length discrepancy, ligamentous laxity, or because of muscular weakness or tightness in the gastrocnemius and soleus muscles. Pronation can be influenced by sources outside of the body as well. Shoes have been shown to significantly influence pronation. Hintermann states that the same person can have different amounts of pronation just by using different running shoes. It is easily possible that the maximal ankle joint eversion movement is 31 degrees for one and 12 degrees for another running shoe.
Symptoms
With over pronation, sufferers are most likely to experience pain through the arch of the foot. A lack of stability is also a common complaint. Over pronation also causes the foot to turn outward during movement at the ankle, causing sufferers to walk along the inner portion of the foot. This not only can deliver serious pain through the heel and ankle, but it can also be the cause of pain in the knees or lower back as well. This condition also causes the arch to sink which places stress on the bones, ligaments, and tendons throughout the foot. This may yield other common conditions of foot pain such as plantar fasciitis and heel spurs.
Diagnosis
To easily get an idea of whether a person overpronates, look at the position and condition of certain structures in the feet and ankles when he/she stands still. When performing weight-bearing activities like walking or running, muscles and other soft tissue structures work to control gravity's effect and ground reaction forces to the joints. If the muscles of the leg, pelvis, and feet are working correctly, then the joints in these areas such as the knees, hips, and ankles will experience less stress. However, if the muscles and other soft tissues are not working efficiently, then structural changes and clues in the feet are visible and indicate habitual overpronation.
Non Surgical Treatment
Anti-Pronation Insoles provide a unique foot support system that aligns the lower body. The major cause of foot and leg pain is over pronation (rolling over of the feet) which causes excessive pressure on the muscles, ligaments and bones of the lower body. Running insoles treat the underlying cause of over pronation and prevent future occurrences of the associated foot or leg condition. A project conducted at the NIKE Sport Research Laboratory studied the effects of orthotics on rear foot movement in running. Nine well-trained runners who wore orthotics were chosen as subjects. The results of the study indicated that orthotics reduced rear foot movement by roughly one degree or approximately nine percent of the amount found in runners not using orthotics. The average reduction of the maximum velocity of pronation was fifteen percent. Thus this study indicates that orthotics and insoles control over pronation which will treat and prevent many sporting injuries.
Surgical Treatment
Depending on the severity of your condition, your surgeon may recommend one or more treatment options. Ultimately, however, it's YOUR decision as to which makes the most sense to you. There are many resources available online and elsewhere for you to research the various options and make an informed decision.
Ways To Treat Severs Disease?
Overview
Sever?s disease, also known as calcaneal apophysitis or Osgood-Schlatter syndrome of the foot. This traction apophysitis is secondary to repetitive microtraumata or overuse of the heel in young athletes. The calcaneus is situated at the most plantar posterior aspect of the foot. The Achilles tendon inserts to the lower, posterior and slightly medial aspect of the calcaneus. The plantar fascia originates from the medial tubercle on the plantar aspect of the calcaneus. Proximal to the epiphysis is the apophysis, where the Achilles tendon actually inserts. The calcaneal growth plate and apophysis are situated in an area subject to high stress from the plantar and Achilles tendon.
Causes
Predisposing Hereditary Factors: These are a biomechanical defect that one may be born with, which increases the chances of developing Sever's Disease. Short Achilles Tendon, When the Achilles Tendon is short from birth, it will exaggerate the tightness of this tendon that occurs during a child's growing years. This makes the pull of the Achilles Tendon on the heel's growth plate more forceful than normal, causing inflammation and pain, and eventually Sever's Disease. Short Leg Syndrome, When one leg is shorter than the other, the foot on the short leg must plantar flex (the foot and toes bend down) in order to reach the ground. In this way, the body tries to equalize the length of the legs. In order for the foot to plantar flex, the Achilles Tendon must pull on the heel with greater force than if the leg was a normal length. Thus the heel on the short leg will be more susceptible to Sever's Disease during the foot's growing years. Pronation. Is a biomechanical defect of the foot that involves a rolling outward of the foot at the ankle, so that when walking, the inner side of the heel and foot bears more of the body's weight than is normal (click here for more information about pronation). Pronation thus causes the heel to be tilted or twisted. In order for the Achilles Tendon to attach to the heel, it must twist to reach its normal attachment site. This will shorten or tighten the Achilles Tendon and increase the force of its pull on the heel's growth plate. This will increase the tightness of the Achilles Tendon during the foot's growing years, and may help to initiate bouts of Sever's Disease. Flat Arches and High Arches. Both of these biomechanical foot defects effect the pitch, or angle of the heel within the foot. When the heel is not positioned normally within the foot due to the height of the arch, the Achilles Tendon's attachment to the heel is affected. This may produce a shortening or tightening of the Achilles Tendon, which increases the force of its pull on the heel's growth plate. During the foot's growing years, abnormal arch height may contribute to the onset of Sever's Disease.
Symptoms
Sever's disease causes pain and tenderness in the back and bottom of the heel when walking or standing, and the heel is painful when touched. It can occur in one or both feet.
Diagnosis
Sever?s disease is diagnosed based on a doctor?s physical examination of the lower leg, ankle, and foot. If the diagnosis is in question, the doctor may order x-rays or an MRI to determine if there are other injuries that may be causing the heel pain.
Non Surgical Treatment
The doctor will talk with you about the best treatment plan for your child. As instructed, your child will Ice the heel 3-4 times a day for 15-20 minutes at a time. Use an ice pack or bag of frozen peas, or something similar. Never put ice directly on your child's skin. A thin cloth or towel should be between your child?s skin and the ice pack. Take anti-inflammatory medication, such as ibuprofen, as directed. Decrease the amount of running and jumping he or she does. Stretch the heels and calves, as instructed by the doctor. Regular stretching can help prevent Sever?s from coming back. Use a ?heel cup? or a cushioned shoe insert that takes pressure off the heel. In some cases, a cast is placed on the foot and worn for several weeks.
Exercise
The following exercises are commonly prescribed to patients with Severs disease. You should discuss the suitability of these exercises with your physiotherapist prior to beginning them. Generally, they should be performed 1 - 3 times daily and only provided they do not cause or increase symptoms. Your physiotherapist can advise when it is appropriate to begin the initial exercises and eventually progress to the intermediate, advanced and other exercises. As a general rule, addition of exercises or progression to more advanced exercises should take place provided there is no increase in symptoms. Calf Stretch with Towel. Begin this stretch in long sitting with your leg to be stretched in front of you. Your knee and back should be straight and a towel or rigid band placed around your foot as demonstrated. Using your foot, ankle and the towel, bring your toes towards your head as far as you can go without pain and provided you feel no more than a mild to moderate stretch in the back of your calf, Achilles tendon or leg. Hold for 5 seconds and repeat 10 times at a mild to moderate stretch provided the exercise is pain free. Calf Stretch with Towel. Begin this exercise with a resistance band around your foot and your foot and ankle held up towards your head. Slowly move your foot and ankle down against the resistance band as far as possible and comfortable without pain, tightening your calf muscle. Very slowly return back to the starting position. Repeat 10 - 20 times provided the exercise is pain free. Once you can perform 20 repetitions consistently without pain, the exercise can be progressed by gradually increasing the resistance of the band provided there is no increase in symptoms. Bridging. Begin this exercise lying on your back in the position demonstrated. Slowly lift your bottom pushing through your feet, until your knees, hips and shoulders are in a straight line. Tighten your bottom muscles (gluteals) as you do this. Hold for 2 seconds then slowly lower your bottom back down. Repeat 10 times provided the exercise is pain free.
Sever?s disease, also known as calcaneal apophysitis or Osgood-Schlatter syndrome of the foot. This traction apophysitis is secondary to repetitive microtraumata or overuse of the heel in young athletes. The calcaneus is situated at the most plantar posterior aspect of the foot. The Achilles tendon inserts to the lower, posterior and slightly medial aspect of the calcaneus. The plantar fascia originates from the medial tubercle on the plantar aspect of the calcaneus. Proximal to the epiphysis is the apophysis, where the Achilles tendon actually inserts. The calcaneal growth plate and apophysis are situated in an area subject to high stress from the plantar and Achilles tendon.
Causes
Predisposing Hereditary Factors: These are a biomechanical defect that one may be born with, which increases the chances of developing Sever's Disease. Short Achilles Tendon, When the Achilles Tendon is short from birth, it will exaggerate the tightness of this tendon that occurs during a child's growing years. This makes the pull of the Achilles Tendon on the heel's growth plate more forceful than normal, causing inflammation and pain, and eventually Sever's Disease. Short Leg Syndrome, When one leg is shorter than the other, the foot on the short leg must plantar flex (the foot and toes bend down) in order to reach the ground. In this way, the body tries to equalize the length of the legs. In order for the foot to plantar flex, the Achilles Tendon must pull on the heel with greater force than if the leg was a normal length. Thus the heel on the short leg will be more susceptible to Sever's Disease during the foot's growing years. Pronation. Is a biomechanical defect of the foot that involves a rolling outward of the foot at the ankle, so that when walking, the inner side of the heel and foot bears more of the body's weight than is normal (click here for more information about pronation). Pronation thus causes the heel to be tilted or twisted. In order for the Achilles Tendon to attach to the heel, it must twist to reach its normal attachment site. This will shorten or tighten the Achilles Tendon and increase the force of its pull on the heel's growth plate. This will increase the tightness of the Achilles Tendon during the foot's growing years, and may help to initiate bouts of Sever's Disease. Flat Arches and High Arches. Both of these biomechanical foot defects effect the pitch, or angle of the heel within the foot. When the heel is not positioned normally within the foot due to the height of the arch, the Achilles Tendon's attachment to the heel is affected. This may produce a shortening or tightening of the Achilles Tendon, which increases the force of its pull on the heel's growth plate. During the foot's growing years, abnormal arch height may contribute to the onset of Sever's Disease.
Symptoms
Sever's disease causes pain and tenderness in the back and bottom of the heel when walking or standing, and the heel is painful when touched. It can occur in one or both feet.
Diagnosis
Sever?s disease is diagnosed based on a doctor?s physical examination of the lower leg, ankle, and foot. If the diagnosis is in question, the doctor may order x-rays or an MRI to determine if there are other injuries that may be causing the heel pain.
Non Surgical Treatment
The doctor will talk with you about the best treatment plan for your child. As instructed, your child will Ice the heel 3-4 times a day for 15-20 minutes at a time. Use an ice pack or bag of frozen peas, or something similar. Never put ice directly on your child's skin. A thin cloth or towel should be between your child?s skin and the ice pack. Take anti-inflammatory medication, such as ibuprofen, as directed. Decrease the amount of running and jumping he or she does. Stretch the heels and calves, as instructed by the doctor. Regular stretching can help prevent Sever?s from coming back. Use a ?heel cup? or a cushioned shoe insert that takes pressure off the heel. In some cases, a cast is placed on the foot and worn for several weeks.
Exercise
The following exercises are commonly prescribed to patients with Severs disease. You should discuss the suitability of these exercises with your physiotherapist prior to beginning them. Generally, they should be performed 1 - 3 times daily and only provided they do not cause or increase symptoms. Your physiotherapist can advise when it is appropriate to begin the initial exercises and eventually progress to the intermediate, advanced and other exercises. As a general rule, addition of exercises or progression to more advanced exercises should take place provided there is no increase in symptoms. Calf Stretch with Towel. Begin this stretch in long sitting with your leg to be stretched in front of you. Your knee and back should be straight and a towel or rigid band placed around your foot as demonstrated. Using your foot, ankle and the towel, bring your toes towards your head as far as you can go without pain and provided you feel no more than a mild to moderate stretch in the back of your calf, Achilles tendon or leg. Hold for 5 seconds and repeat 10 times at a mild to moderate stretch provided the exercise is pain free. Calf Stretch with Towel. Begin this exercise with a resistance band around your foot and your foot and ankle held up towards your head. Slowly move your foot and ankle down against the resistance band as far as possible and comfortable without pain, tightening your calf muscle. Very slowly return back to the starting position. Repeat 10 - 20 times provided the exercise is pain free. Once you can perform 20 repetitions consistently without pain, the exercise can be progressed by gradually increasing the resistance of the band provided there is no increase in symptoms. Bridging. Begin this exercise lying on your back in the position demonstrated. Slowly lift your bottom pushing through your feet, until your knees, hips and shoulders are in a straight line. Tighten your bottom muscles (gluteals) as you do this. Hold for 2 seconds then slowly lower your bottom back down. Repeat 10 times provided the exercise is pain free.
Achilles Tendon Rupture Non Surgical Recovery Timeline
Overview
 Many of the muscles that move the foot are found in the lower leg. These muscles attach via tendons to various bones in the foot. The main muscles that move the foot downwards (plantar flex the foot) and propel the body forward are the calf muscles (gastrocnemius and soleus muscles). These muscles are connected to the heel bone (calcaneus) by the "rope like" Achilles tendon. Achilles tendon rupture is the term used to describe a complete tear of the Achilles tendon. The most common site for Achilles tendon rupture to occur is an area 2 - 6 cm. (1 - 2.5 in.) above where the tendon attaches to the calcaneus.
Many of the muscles that move the foot are found in the lower leg. These muscles attach via tendons to various bones in the foot. The main muscles that move the foot downwards (plantar flex the foot) and propel the body forward are the calf muscles (gastrocnemius and soleus muscles). These muscles are connected to the heel bone (calcaneus) by the "rope like" Achilles tendon. Achilles tendon rupture is the term used to describe a complete tear of the Achilles tendon. The most common site for Achilles tendon rupture to occur is an area 2 - 6 cm. (1 - 2.5 in.) above where the tendon attaches to the calcaneus.
Causes
A rupture occurs when a patient overstretches the Achilles tendon, an act which causes it to tear partially or completely. Achilles tendon ruptures can occur during athletic play or any time the tendon is stretched in an unexpected way.
Symptoms
Symptoms include a sudden sharp pain in the achilles tendon which is often described as if being physically struck by an object or implement. A loud snapping noise or bang may also be heard at the time. A gap of 4 to 5 cm in the tendon can be felt which may be less obvious later as swelling increases. After a short while the athlete may be able to walk again but without the power to push off with the foot. There will be a significant loss of strength in the injured leg and the patient will be unable to stand on tip toes. There may be considerable swelling around the achilles tendon and a positive result for Thompson's test can help confirm the diagnosis.
Diagnosis
During the physical exam, your doctor will inspect your lower leg for tenderness and swelling. In many cases, doctors can feel a gap in your tendon if a complete rupture has occurred. Achilles tendon rupture can be diagnosed reliably with clinical examination, but if there?s a question about the extent of your Achilles tendon injury then your doctor may order a magnetic resonance imaging (MRI) scan.
Non Surgical Treatment
There are two treatment options available which are non-operative and operative. Non-operative treatment involves the use initially of a below-knee plaster with the foot held fully bent downwards. This usually stays in place for 2 weeks then is changed for a brace(this is a boot from the knee down to the toes with Velcro straps) which should be worn day and night. The brace will be regularly altered to allow the foot to come up to a more neutral position. The brace will be on for a further 6 weeks. After the 8 weeks you will be referred for physiotherapy to regain movement and calf strength but will probably need to wear the brace during the day for a further 4 weeks. Non-operative treatment avoids the risks of surgery but the risk of the tendon re-rupturing, which normally occurs within 3 months of discarding the brace, is 10%. 
Surgical Treatment
Regaining Achilles tendon function after an injury is critical for walking. The goal of Achilles tendon repair is to reconnect the calf muscles with the heel bone to restore push-off strength. Those best suited for surgical repair of an acute or chronic Achilles tendon rupture include healthy, active people who want to return to activities such as jogging, running, biking, etc. Even those who are less active may be candidates for surgical repair. Non-operative treatment may also be an option. The decision to operate should be discussed with your orthopaedic foot and ankle surgeon.
Prevention
Prevention centers on appropriate daily Achilles stretching and pre-activity warm-up. Maintain a continuous level of activity in your sport or work up gradually to full participation if you have been out of the sport for a period of time. Good overall muscle conditioning helps maintain a healthy tendon.